By Anna-Marie Schmidt, MM, DC, and Robert Vining, DC, DHSc
Practitioners use symptoms to guide clinical evaluation and treatment. For example, chest pain on exertion suggests possible need for cardiac evaluation. Pain is a symptom we are trained to explore by asking questions such as, “How severe is your pain?” and “Where is the pain located?” We ask these questions because the answers help point us in the direction of a diagnosis. However, pain symptoms are sometimes unreliable. Such instances can lead to misdiagnosis, frustration, questioning the legitimacy of a symptom or a suspicion of malingering.1
For people experiencing chronic pain, symptom characteristics may not match patterns found in acute cases.1 The physiological basis for this alternate pain experience can be the result of peripheral or central sensitization. Sensitization (whether peripheral or central) is a process whereby neurons learn to become more responsive to nociceptive signals and/or translate stimuli that don’t normally produce pain into those that do.2
Hyperalgesia and Allodynia
Metaphorically, pain can be thought of as part of the body’s alarm system designed to become extra sensitive under certain circumstances.3,4 Following acute trauma increased sensitivity serves as a reminder to protect injured tissues. However, when sensitization persists beyond a normal period,5,6 pain can be perceived from both noxious and non-noxious stimuli, the result of adaptive changes within the Central Nervous System (CNS).6 This can be observed clinically as hyperalgesia (e.g., increased response to pinprick) and allodynia (e.g., pain response to light touch such as a cotton swab).6,7 Figures 1 and 2 describe changes in sensory pathways leading to sensitization.6–10
Figure 1: Hyperalgesia2,6–10
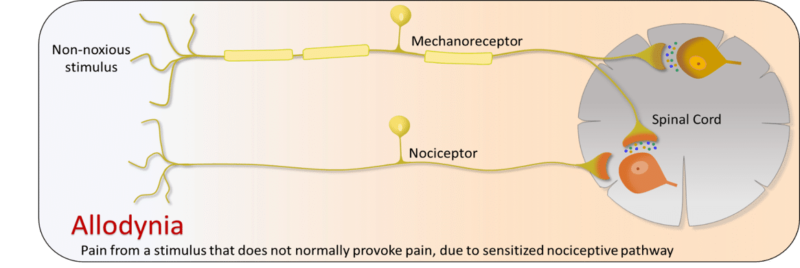
Figure 2. Allodynia2,6–10

Identifying Sensitization
Nervous system changes causing sensitization occur along a continuum making symptoms variable and sometimes unique. The presence of hyperalgesia and/or allodynia provide indirect exam evidence of sensitization.7,8,11 The International Association for the Study of Pain (IASP) emphasizes three major criteria for identifying likely central sensitization.6,12
- Severity of the experience is disproportionate to the nature and extent of the injury or pathology13
Meeting this criterion occurs when the clinical evidence for the amount of injury/dysfunction is substantially less than a patient’s subjective experience. We can observe this when there is an exaggerated response to pain-provoking tests.12,13
- Neuroanatomically illogical pain pattern13
The presence of bilaterally symmetrical pain, pain that alternately varies in anatomical location and symptoms widely spread over large areas, can potentially be neuroanatomically illogical, because they are not consistent nor do they follow typical nerve distribution patterns.12,13 However, clinical interpretation accounting for other explanations, such as fever, visceral symptoms, and co-existing conditions is needed.
- Hypersensitivity of senses unrelated to the musculoskeletal system13
Sensitization can cause abnormally increased responses to stimuli other than pain. This potentially includes increased sensitivity to chemicals (odors, medications), temperature, sound, weather characteristics and emotional stressors. Assessing this criterion can begin with asking persons questions about hypersensitivity to light, sound, smell and temperature.12,13
Clinical Implications
Sensitization usually occurs when pain has been present long enough to allow nervous system adaptation.6 This means most people with sensitization have chronic pain. However, adaptation is variable and it is inaccurate to assume that all people with chronic pain have sensitization.14
Sensitization can and does co-occur with other conditions. Comorbidities and sensitization can negatively impact each other. Additional factors, sometimes called lifestyle factors, can similarly impact and be impacted by sensitization. Such factors include:5
- Negative illness beliefs, including negative emotions and pain-related memories, have a shared neural connection with areas facilitating chronic pain and sensitization.15
- Unhealthy diet is suggested to be closely linked to sensitization through inflammatory mediators.5
- Physical inactivity can be due to negative illness beliefs resulting from a dysfunctional pain response (hyperalgesia) to exercise.16
- Poor sleep is a common comorbidity of chronic pain. Lacking sleep can lead to low-grade inflammation, something linked to hyperalgesia and anxiety.15
Not understanding how and why sensitization occurs can lead to misinterpreting symptoms and developing ineffective, or even counterproductive management strategies.5 Education is therefore considered a critical component of any management approach.15 Part 2 of this series describes key aspects of educationally-oriented management strategies and addresses other factors important in helping patients with sensitization.
Learn about management strategies for sensitization in Part 2.
Anna-Marie Schmidt MM, DC is a Post-Doctoral Research Scholar at the Palmer Center for Chiropractic Research, Palmer College of Chiropractic.
Robert Vining, DC, DHSc is Associate Dean of Clinical Research at the Palmer Center for Chiropractic Research, Palmer College of Chiropractic.
References
- Tuck NL, Johnson MH, Bean DJ. You’d Better Believe It: The Conceptual and Practical Challenges of Assessing Malingering in Patients With Chronic Pain. The Journal of Pain. 2019;20(2):133-145. doi:10.1016/j.jpain.2018.07.002
- IASP Terminology – IASP. IASP Terminology. https://www.iasp-pain.org/Education/Content.aspx?ItemNumber=1698&navItemNumber=576#Sensitization. Published 2017. Accessed November 8, 2019.
- Louw A, Diener I, Landers MR, Puentedura EJ. Preoperative pain neuroscience education for lumbar radiculopathy: a multicenter randomized controlled trial with 1-year follow-up. Spine. 2014;39(18):1449-1457. doi:10.1097/BRS.0000000000000444
- Butler DS, Moseley GL. Explain Pain: (Revised and Updated, 2nd Edition). Noigroup Publications; 2013.
- Nijs J, Leysen L, Vanlauwe J, et al. Treatment of central sensitization in patients with chronic pain: time for change? Expert Opinion on Pharmacotherapy. 2019;20(16):1961-1970. doi:10.1080/14656566.2019.1647166
- Sanzarello I, Merlini L, Rosa MA, et al. Central sensitization in chronic low back pain: A narrative review. Journal of Back and Musculoskeletal Rehabilitation. 2016;29(4):625-633. doi:10.3233/BMR-160685
- Jensen TS, Finnerup NB. Allodynia and hyperalgesia in neuropathic pain: clinical manifestations and mechanisms. The Lancet Neurology. 2014;13(9):924-935. doi:10.1016/S1474-4422(14)70102-4
- Arendt‐Nielsen L, Morlion B, Perrot S, et al. Assessment and manifestation of central sensitisation across different chronic pain conditions. European Journal of Pain. 2018;22(2):216-241. doi:10.1002/ejp.1140
- Woolf CJ. Central sensitization: Implications for the diagnosis and treatment of pain. Pain. 2011;152(3 Suppl):S2-15. doi:10.1016/j.pain.2010.09.030
- Kandel E, Schwartz J, Jessell T. Principles of Neural Science, Fourth Edition. Fourth. McGraw-Hill Companies,Incorporated; 2000.
- den Bandt HL, Paulis WD, Beckwée D, Ickmans K, Nijs J, Voogt L. Pain Mechanisms in Low Back Pain: A Systematic Review With Meta-analysis of Mechanical Quantitative Sensory Testing Outcomes in People With Nonspecific Low Back Pain. J Orthop Sports Phys Ther. 2019;49(10):698-715. doi:10.2519/jospt.2019.8876
- Nijs J, Apeldoorn A, Hallegraeff H, et al. Low Back Pain: Guidelines for the Clinical Classification of Predominant Neuropathic, Nociceptive, or Central Sensitization Pain. Pain Physician. 2015;18(3):333-346.
- Nijs J, Torres-Cueco R, van Wilgen CP, et al. Applying modern pain neuroscience in clinical practice: criteria for the classification of central sensitization pain. Pain Physician. 2014;17(5):447-457.
- Tayor AJ, Kerry R. When Chronic Pain Is Not “Chronic Pain”: Lessons From 3 Decades of Pain. J Orthop Sports Phys Ther. 2017;47(8):515-517. doi:10.2519/jospt.2017.0606
- Nijs J, Clark J, Malfliet A, et al. In the spine or in the brain? Recent advances in pain neuroscience applied in the intervention for low back pain. Clin Exp Rheumatol. 2017;35 Suppl 107(5):108-115.
- Nijs J, Kosek E, Van Oosterwijck J, Meeus M. Dysfunctional endogenous analgesia during exercise in patients with chronic pain: to exercise or not to exercise? Pain Physician. 2012;15(3 Suppl):ES205-213.