Part of the Evidence in Action series by Palmer College of Chiropractic
The American College of Physicians (ACP) recently release a clinical practice guideline for noninvasive treatments for low back pain.1 The goal of this guideline is to inform care decisions by systematically evaluating and summarizing available scientific evidence for treating acute, subacute and chronic low back pain. Many treatments used by doctors of chiropractic such as spinal manipulation, superficial heat, acupuncture, motor control exercise and low level laser are included as recommended first-line treatments.2
Creating this guideline began with an exhaustive review of the literature for articles reporting clinical trial data for noninvasive interventions. Literature reviews are most valuable within the first few years of publication. New evidence has the potential to alter recommendations, thus, periodic updated reviews are needed. The ACP guideline was based on a systematic review conducted by the Agency for Healthcare Research and Quality (AHRQ), as shown in Figure 1.
Figure 1. Major steps in the ACP guideline development process

Interventions recommended by this guideline are categorized by strength and quality, which describe the various levels of evidence supporting each treatment. Thus, understanding how the categories of quality and strength are decided is necessary to accurately interpret recommendations. Fortunately, Qaseem and colleagues describe the evidence categorization process in a separate publication.6
How Evidence Quality Is Decided
Evaluating quality of evidence supporting a guideline recommendation includes two steps. The first is determining how confidently clinical trial evidence demonstrates a true effect of the treatment under study. The second involves estimating the potential for future studies to change the observed treatment effects. Treatments with similar effects from multiple studies generate higher levels of confidence than those with conflicting results or when only a single clinical trial has been conducted. Figure 2 graphically displays the criteria used in evidence quality decisions.
High-quality
Consistent findings across multiple studies and/or methodologically rigorous studies directly applicable to patient care are required for designating high-quality evidence. If both consistency and applicability suggest further research is unlikely to change the rater’s confidence in the treatment effect the evidence is rated as high-quality.
Moderate-quality
If the estimate of treatment effect will probably change with future research, the evidence is graded as moderate-quality. Moderate-quality evidence is characterized by studies that may show similar results in populations that are slightly different, studies with low numbers of participants, or where there is the potential for biased assessment of result, among others.
Low-quality
Evidence is rated as low-quality when conflicting results give low confidence in the effect of the treatment and/or future research will likely have a substantial effect on the confidence of the treatment effect.
Figure 2. Evidence quality decisions

How Recommendation Strength Is Decided
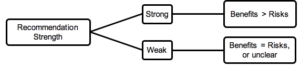
Risk vs. benefit comparisons determine recommendation strength. A strong recommendation indicates benefits of treatment clearly outweigh risks. A weak recommendation indicates treatments have equivalent or as yet unclear risk compared with benefit(s). Figure 3 graphically displays the criteria used in recommendation strength decisions.
Figure 3. Recommendation strength decisions

Implications
Guidelines do not provide enough details to determine which treatment or combination of treatments to employ in individual cases. Nevertheless, guidelines carry important implications for both patients and clinicians. The ACP guideline suggests most patients will seek strongly recommended treatments, should discuss them with their physician, and that clinicians should be providing recommended treatments to most patients.
For patients with acute or subacute low back pain, the ACP guideline suggests it is the physician’s responsibility to:
- Reassure patients that there is a high likelihood of symptom improvement within a few weeks, with or without treatment
- Avoid unnecessary diagnostic testing and treatment
- Advise patients to remain active as tolerated
- Provide self-care options
- Facilitate shared decision-making
- Recommend treatment based on patient preference, treatment effectiveness, risks, costs and availability
According to a 2010 survey, 71% of chiropractors report that they use hot pack/moist heat, while 63% recommended bed rest.2 While it is not clear how often survey respondents use these treatments or the conditions for which they are applied, current evidence suggests that for low back pain, clinicians should not consider bed rest as a treatment. In contrast, heat therapy carries a strong recommendation suggesting this treatment should be considered as part of a potential management strategy.
The ACP guideline does not obligate clinicians to offer recommended treatments. However, because guidelines are based on scientific evidence, providers have a responsibility to be both informed and able to communicate about recommended treatments with patients. Patients may not be aware of what treatments are supported by evidence or how firmly they are supported, which are important factors when making informed decisions about care.
Dr. Vining is associate professor and senior research clinician at the Palmer Center for Chiropractic Research, Palmer College of Chiropractic, Davenport, Iowa.
Dr. Shannon is a clinical research fellow at the Palmer Center for Chiropractic Research, Palmer College of Chiropractic, Davenport, Iowa.
References
- Qaseem A, Wilt TJ, McLean RM, Forciea MA. Noninvasive Treatments for Acute, Subacute, and Chronic Low Back Pain: A Clinical Practice Guideline from the American College of Physicians. Ann Intern Med, 2017; Feb 14.
- National Board of Chiropractic Examiners Practice Analysis of Chiropractic 2010. National Board of Chiropractic Examiners 2010.
- Chou R, Deyo R, Friedly J, et al. Noninvasive Treatments for Low Back Pain. Comparative Effectiveness Reviews, No. 169. Prepared by the Pacific Northwest Evidence-based Practice Center under Contract No. 290-2012-00014-I.; 2017; Feb. Report No.: 16-EHC004-EF.
- Chou R, Deyo R, Friedly J, Skelly A, Hashimoto R, Weimer M, et al. Nonpharmacologic Therapies for Low Back Pain: A Systematic Review for an American College of Physicians Clinical Practice Guideline. Ann Intern Med, 2017; Feb 14.
- Chou R, Deyo R, Friedly J, Skelly A, Weimer M, Fu R, et al. Systemic Pharmacologic Therapies for Low Back Pain: A Systematic Review for an American College of Physicians Clinical Practice Guideline. Ann Intern Med, 2017, Apr 4; 166(7): 480-92.
- Qaseem A, Snow V, Owens DK, Shekelle P. The development of clinical practice guidelines and guidance statements of the American College of Physicians: summary of methods. Ann Intern Med, 2010 Aug 3; 153(3):194-9.