By Kara Shannon, DC, and Robert Vining, DC
Effective communication is a known factor in creating a strong therapeutic relationship.1 Therapeutic relationships can facilitate patient adherence to therapy, satisfaction with care and improved outcomes; they have also been associated with reduced malpractice claims.2–7 This article addresses aspects of communication which are key to building therapeutic relationships in chiropractic practice.
A Dynamic Process
During clinical encounters doctors and patients alternately send information while simultaneously playing a secondary role as information receiver (Figure 1). The information exchange occurs both verbally and non-verbally. Using this model as a reference, one might ask: Can this help us understand and potentially improve doctor-patient communication? Research evidence suggests the answer is likely “yes.”

Figure 1. (above) Conceptual model of a two-way dynamic communication process where both parties send and receive information simultaneously.
The Consultation
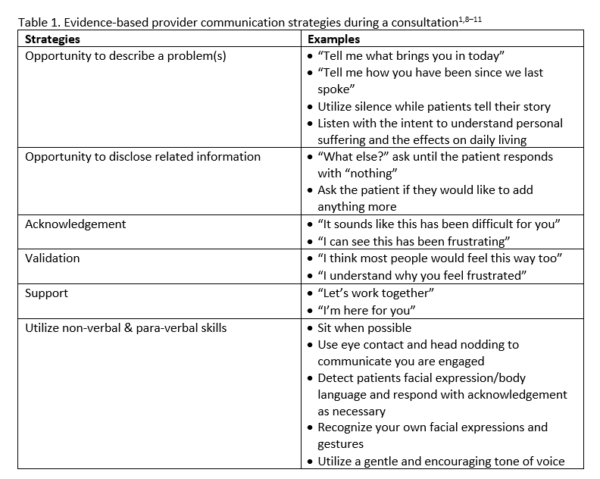
Whether conducting an initial or follow-up visit, there is typically a set time for obtaining problem-focused history information. During the consultation stage of a clinical encounter, the doctor’s main purpose is to obtain (receive) information needed to direct follow-up activities. Important clinical information can be obtained verbally or through observation of facial expression, inflection, postures, etc. Table 1 describes key elements consistent with a biopsychosocial approach that may support an effective information exchange.
An Example Case Study
After asking standard history questions a doctor conducted an exam of the low back. Following the exam, the doctor explained the working diagnosis. At the opportunity for questions, the patient asked: “Do you think falling off a ladder could cause this?” This question made the doctor aware of the recent fall. Given this new information the doctor inquired further, which led to uncovering the cause of the fall, light-headedness, and a diagnosis of hypotension. A referral to reassess anti-hypertensive medication was generated.
Fortunately, in the case described above, key information about the patient’s fall was uncovered during the visit. But, why wasn’t it discovered earlier? It could be that the doctor did not provide the right opportunity for the patient to fully explain the problem. In this example, simply asking “what else” until the patient’s history and questions were exhausted, could have led to earlier disclosure of the fall and the hypotension diagnosis.
Secondary Messages
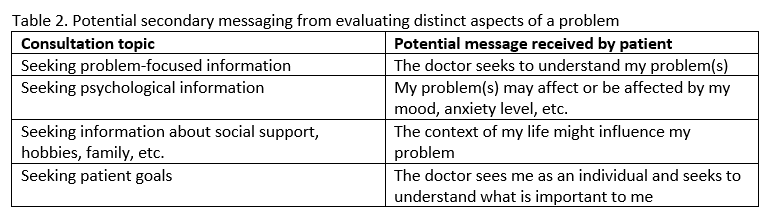
Secondary messages are sent or received alongside other forms of communication. Ideally, non-verbal and paraverbal communication (e.g., facial expressions, voice inflection) facilitate healthy therapeutic relationships.11 Table 2 displays other positive secondary messages patients can potentially receive when clinically evaluating different aspects of a problem.

Self-reflection
As providers, we have a responsibility to facilitate an environment that fosters an effective information exchange with patients. Understanding our roles as both information sender and receiver may be enhanced through self-reflection. We conclude this topic by offering a critical self-reflection checklist (Table 3) with items drawn from literature reviewed during the development of this article. 1,9–17 The checklist is a tool designed to help self-reflect on key communication concepts that facilitate professional patient-centered communication using a biopsychosocial approach.

Kara Shannon, DC is an Adjunct Faculty member at Palmer College of Chiropractic and a Research Clinician at the Palmer Center for Chiropractic Research, Davenport IA.
Robert Vining, DC, DHSc is a Professor and Associate Dean of Clinical Research at the Palmer Center for Chiropractic Research, Palmer College of Chiropractic.
References
- Pinto RZ, Ferreira ML, Oliveira VC, et al. Patient-centred communication is associated with positive therapeutic alliance: a systematic review. J Physiother. 2012;58(2):77-87. doi:10.1016/S1836-9553(12)70087-5
- Babatunde F, MacDermid J, MacIntyre N. Characteristics of therapeutic alliance in musculoskeletal physiotherapy and occupational therapy practice: a scoping review of the literature. BMC Health Serv Res. 2017;17(1):375. doi:10.1186/s12913-017-2311-3
- Moore AJ, Holden MA, Foster NE, Jinks C. Therapeutic alliance facilitates adherence to physiotherapy-led exercise and physical activity for older adults with knee pain: a longitudinal qualitative study. J Physiother. 2020;66(1):45-53. doi:10.1016/j.jphys.2019.11.004
- Boissy A, Windover AK, Bokar D, et al. Communication Skills Training for Physicians Improves Patient Satisfaction. J Gen Intern Med. 2016;31(7):755-761. doi:10.1007/s11606-016-3597-2
- Kinney M, Seider J, Beaty AF, Coughlin K, Dyal M, Clewley D. The impact of therapeutic alliance in physical therapy for chronic musculoskeletal pain: A systematic review of the literature. Physiother Theory Pract. September 2018:1-13. doi:10.1080/09593985.2018.1516015
- Kelley JM, Kraft-Todd G, Schapira L, Kossowsky J, Riess H. The influence of the patient-clinician relationship on healthcare outcomes: a systematic review and meta-analysis of randomized controlled trials. PloS One. 2014;9(4):e94207. doi:10.1371/journal.pone.0094207
- Melonas JM, McNary AL. Taking action to avoid recurring risks in medical professional liability claims. Neurology. 2010;75(18 Suppl 1):S45-51. doi:10.1212/WNL.0b013e3181fc284c
- Littell RD, Kumar A, Einstein MH, Karam A, Bevis K. Advanced communication: A critical component of high quality gynecologic cancer care: A Society of Gynecologic Oncology evidence based review and guide. Gynecol Oncol. 2019;155(1):161-169. doi:10.1016/j.ygyno.2019.07.026
- Patel S, Pelletier-Bui A, Smith S, et al. Curricula for empathy and compassion training in medical education: A systematic review. PloS One. 2019;14(8):e0221412. doi:10.1371/journal.pone.0221412
- Smith RC, Fortin AH, Dwamena F, Frankel RM. An evidence-based patient-centered method makes the biopsychosocial model scientific. Patient Educ Couns. 2013;91(3):265-270. doi:10.1016/j.pec.2012.12.010
- Ranjan P, Kumari A, Chakrawarty A. How can Doctors Improve their Communication Skills? J Clin Diagn Res JCDR. 2015;9(3):JE01-04. doi:10.7860/JCDR/2015/12072.5712
- Brown-Johnson C, Schwartz R, Maitra A, et al. What is clinician presence? A qualitative interview study comparing physician and non-physician insights about practices of human connection. BMJ Open. 2019;9(11):e030831. doi:10.1136/bmjopen-2019-030831
- Chou L, Ranger TA, Peiris W, et al. Patients’ perceived needs for medical services for non-specific low back pain: A systematic scoping review. PloS One. 2018;13(11):e0204885. doi:10.1371/journal.pone.0204885
- Huynh HP, Dicke-Bohmann A. Humble doctors, healthy patients? Exploring the relationships between clinician humility and patient satisfaction, trust, and health status. Patient Educ Couns. 2020;103(1):173-179. doi:10.1016/j.pec.2019.07.022
- Greenfield G, Ignatowicz AM, Belsi A, et al. Wake up, wake up! It’s me! It’s my life! patient narratives on person-centeredness in the integrated care context: a qualitative study. BMC Health Serv Res. 2014;14:619. doi:10.1186/s12913-014-0619-9
- Janisse T, Tallman K. Can All Doctors Be Like This? Seven Stories of Communication Transformation Told by Physicians Rated Highest by Patients. Perm J. 2017;21:16-097. doi:10.7812/TPP/16-097
- Ruben MA, Meterko M, Bokhour BG. Do patient perceptions of provider communication relate to experiences of physical pain? Patient Educ Couns. 2018;101(2):209-213. doi:10.1016/j.pec.2017.08.002